Worrying signs of Endometriosis on Hysterosalpingography
Jan 28, 2020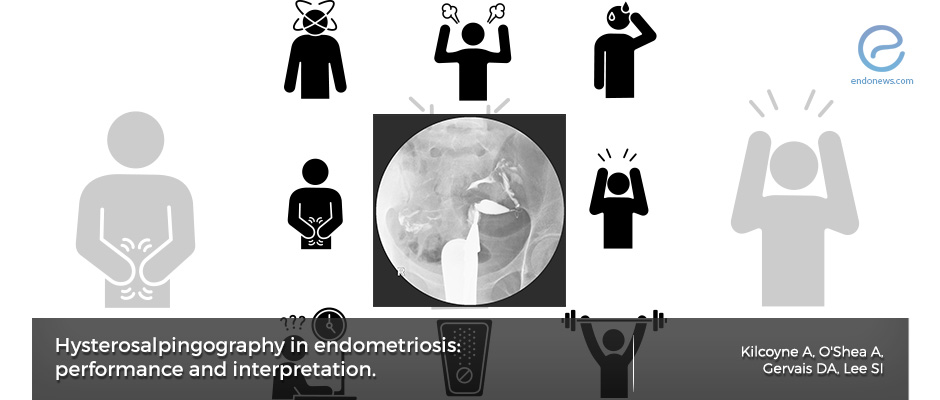
How Hysterosalpingography can help diagnose Endometriosis
Key Points
Importance:
- Infertility workup often includes the use of hysterosalpingography to assess the dynamic and structural aspects of female reproductive anatomy.
- Radiologists should know what findings may suggest endometriosis and patients should be knowledgeable regarding the procedure and its clinical utility.
Highlights:
- The presence of dilated fallopian tubes, lack of contrast spill into the peritoneal cavity, abnormal location of ovaries and/or fallopian tubes, and abnormal uterine contour, septum, and cornua are all findings that may be associated with infertility.
What’s done here:
- The authors discuss when and how HSG should be acquired as well as the findings that may suggest endometriosis-associated pathologies.
Key Results:
- Thorough patient history and patient safety evaluation should be performed before patients are scheduled for an HSG in order to ensure optimal image quality and prevent radiation exposure to an unsuspected pregnancy.
- Possible HSG findings that should be actively assessed include the presence of hydrosalpinx, fallopian tube occlusion, peri-tubal adhesions, deep infiltrating endometriosis as demonstrated by a posterior, midline tubal course, and uterine adenomyosis which may be associated with endometriosis.
- Authors note that while many of these findings are associated with endometriosis, they can also be due to other pathologies. Thus, they suggest that if suspected on HSG, the diagnosis of endometriosis should be confirmed with MRI or laparoscopy.
Limitations:
- This is a review paper regarding associated findings of endometriosis as seen on HSG and includes the authors’ experiences regarding its use during infertility workup.
Lay Summary
Hysterosalpingography (HSG) is an imaging modality that utilizes fluoroscopy in order to evaluate the uterine cavity, fallopian tubes, and adjacent peritoneal cavity by injecting contrast media through the cervical canal. It is an important tool in the work-up of patients who present with infertility.
Thus, radiologists performing and interpreting HSG should be familiar with the findings suspicious for endometriosis-associated infertility in this patient population. A recent article titled, “Hysterosalpingography in endometriosis: performance and interpretation” by Kilcoyne et al. in Abdominal Radiology, aims to describe the acquisition and interpretation of HSG in patients with a focus on endometriosis-associated findings.
The authors first discuss when and how HSG should be performed in patients with infertility. Firstly, consent should be taken after a discussion concerning the possible risks of the procedure including pelvic discomfort, vaginal bleeding, infection, contrast reaction, intrauterine device dislodgement, and the potential for harmful irradiation in the case of patients with an unsuspected pregnancy. Thus, sexually active patients who do not use contraception and are on day 12 or beyond of their menstrual cycle were advised to reschedule the procedure to day 6-11 of their cycle and to use contraception as indicated. This is also helpful in the case of active menses as blood clots may be seen as filling defects in the endometrial cavity. Important also to note that the radiation dose from an HSG is below that of the threshold that determines negligible risk and is thus deemed safe if the patient is not pregnant.
Patients undergoing HSG should know the general method that radiologists use to obtain the best possible image. While the patient is placed in the dorsal lithotomy position, a flexible balloon-tipped catheter is placed into the endocervical canal, inflated, and necessary fluoroscopic images are taken with the use of contrast material. Multiple views are obtained after the initial scout image including an anteroposterior, two oblique views, and ‘en face’ AP view. These views are used to ensure minimal radiation dose while optimizing image quality for evaluation.
The fallopian cornual, isthmic, and especially the ampullary segments should be assessed for tubal obstruction as seen by lack of contrast spill is best seen on oblique views and partial filling of the fallopian tubes. Tubal obstruction can also be seen following surgical procedures and pelvic inflammatory disease due to pelvic adhesions. Hydrosalpinx is seen as an opacified, dilated fallopian tube with an abrupt cutoff and no free spill of contrast into the peritoneal cavity. Tubal occlusion from other causes such as PID, appendicitis, and diverticulitis should also be assessed.
Adenomyosis is generally associated with endometriosis and thus should be assessed during HSG, which may be seen as multiple saccular collections that extend beyond the expected endometrial margin. Assessment of the uterine cavity for Mullerian duct anomalies should include evaluation of the uterine septum and cornua as this can also be a cause of infertility
Authors note that while many of these findings are associated with endometriosis, they can also be due to other pathologies. Thus, if endometriosis is suspected on HSG, the diagnosis should be confirmed with MRI or laparoscopy.
Research Source: https://www.ncbi.nlm.nih.gov/pubmed/31897682
Endometriosis imaging Hysterosalpingography radiology

