Thoracic endometriosis: the most frequent endometriosis involvement outside abdominopelvic cavity
Mar 23, 2022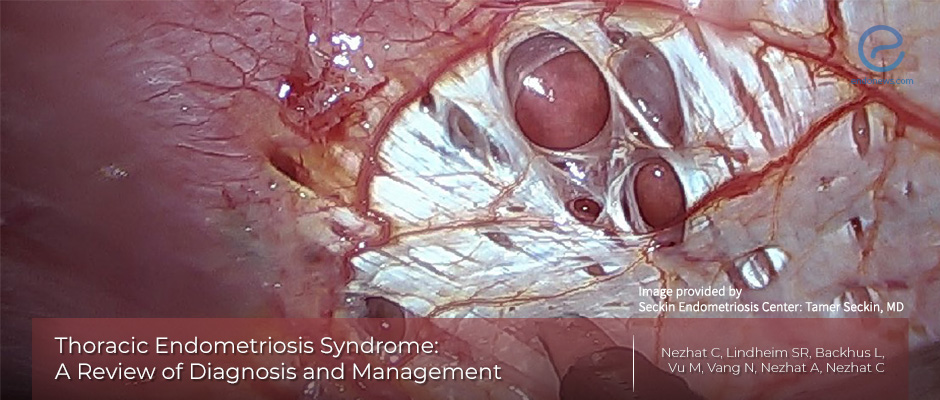
Thoracic and gynecologic surgeons collaborate for treatment of thoracic endometriosis
Key Points
Background:
- Among overall endometriosis, 12% are estimated to be outside the abdominopelvic location, the thoracic cavity being the most frequent.
- Endometriosis within the lung parenchyma or on the diaphragm and pleural surfaces yields a range of manifestations, known as thoracic endometriosis syndrome (TES).
Highlights:
- Useful diagnostic modalities for TES include chest radiographs, computed tomography, magnetic resonance imaging, and bronchoscopy. Similar to pelvic endometriosis, the first-line therapy for TES is medical management aiming to suppress ovarian steroid hormone production.
- However, since thoracic and pelvic endometriosis often exist together, when a patient presents with TES, a multidisciplinary surgical approach to treat both thoracic and pelvic disease in a single procedure is warranted.
Key points:
- Since there is great variability in its presentation, a high level of clinical suspicion is necessary to diagnose and reduce the likelihood of disease progression in TES.
- Videosurgery in contemporary medicine both in diagnosis and management of endometriosis has been a great achievement in preventing incapacitating clinical manifestations.
Conclusion:
- The theories of pathogenesis and epidemiologic observations suggest that thoracic and abdominopelvic endometriosis are often concomitant. In cases of suspected pelvic endometriosis diagnosed and treated by video laparoscopy, the diaphragm should be thoroughly evaluated for evidence of concomitant endometriosis.
- In cases of symptomatic TES where hormonal suppression has not been beneficial or contraindicated, definitive surgical management is ideally performed by gynecologic and thoracic surgeons experienced on the subject.
Lay Summary
Six to ten percent of reproductive-age women are affected by endometriosis, and about 12% are estimated to be outside the abdominopelvic cavity - the most frequent location being the thorax.
Endometriosis within the pulmonary parenchyma or on the diaphragm and pleural surfaces presents different manifestations, collectively known as thoracic endometriosis syndrome.
Besides classic theories of retrograde menstruation, coelomic metaplasia, lymphatic and hematogeneous dissemination in thoracic endometriosis syndrome, a unique prostaglandin theory is also acceptable, where prostaglandin F2α, a potent constrictor of the bronchioles and vasculature increases with menstruation, leading to the constriction of these structures.
Chest radiographs, computed tomography, magnetic resonance imaging, and bronchoscopy are useful modalities for the diagnosis of this unique syndrome.
The first-line therapy for thoracic endometriosis syndrome is also medical, aiming at suppression of ovarian steroid hormone production, however since thoracic and pelvic endometriosis almost always coexist, a multidisciplinary surgical approach to treat both in a single procedure is warranted.
Due to the wide variability in its presentation, a high level of clinical suspicion is important to diagnose and reduce the likelihood of disease progression in thoracic endometriosis syndrome. Videosurgery performed by a multidisciplinary team both in the diagnosis and management of endometriosis has been a great achievement in this regard.
This comprehensive review paper, published by Nezhat et al, appeared in the "Journal of the Society of Laparoendscopic Surgeons".
Research Source: https://www.ncbi.nlm.nih.gov/pubmed/31427853
TES thoracic endometriosis video laparoscopy

