How to Classify Endometriosis for a better and effective evaluation
Aug 5, 2019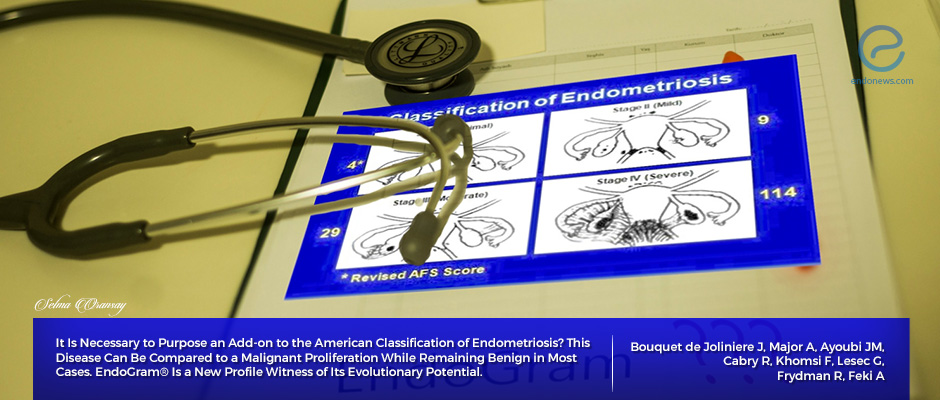
In the current classification system, the stages of the lesions, in terms of their deep molecular biology and their evolution, cannot compare as similar.
Key Points
Highlights:
- To describe peritoneal endometriotic implants, American Society of Reproductive Medicine scored endometriosis quantitatively, from mild to severe, in1996.
- Endometriotic lesions do not all have the same characteristics, and sometimes, even the lesion is small, can create harmful and progressive results that can discredit the above classification.
Importance:
- The phenotype of each endometriosis should be evaluated before starting to treat, just like we need for breast cancer.
- A personalized examination should include vascularization, inflammation, immunity, hormone receptors, proliferation properties.
What's done here:
- Authors proposed to add an "EndoGram" test to improve staging system of endometriosis performed by the American Society of Reproductive Medicine.
- They suggest creating a new therapeutic strategy along with the phenotype of the disease for every individual patient, for a personalized treatment.
Backgrounds:
- Due to the need for a proper classification to evaluate endometriosis, the first attempt was made by ACOSTA in 1973.
- In 1979 AFS (American Fertility Society) create a new classification for endometriosis and revised it in 1985.
- ASRM (American Society of Reproductive Medicine) described the disease at different stages like mild, moderate and severe, given scores for each of them.
- r-ASRM revised ASRM classification is made in 1997 and they added the description of peritoneal implants (white, red and black) to the prior.
- All these classifications are limited by the size and shape of the lesions while they don't give into account the inflammatory phenomena.
- On the other hand, FOATI classification which developed in 1991-1992 turned into FOATI-ARVS in 2010 after revision. ( F=Foci for superficial implants, O= ovarian endometrioma, A= adhesions, T= lesions of the tubal wall, I= Inflammatory appearance and A= adenomyosis RVS= involvement of rectovaginal wall.)
Lay Summary
Endometriosis affects 10% of women in their reproductive period and causes infertility around 40% of women who have the disease. Peritoneal fluid may be one of the factors to facilitate the spread of endometriosis to ovaries, peritoneum and other deep tissues. Small, but progressive lesions may progress more aggressively inside the pelvic space and be more harmful to patient fertility when compared to larger but calm masses of endometriomas.
Joliniere et al., from the Department of Gynecology and Obstetrics in Fribourg Cantonal Hospital, Switzerland, recently shared their concerns about creating a more functional classification for endometriosis than AFS and ASRM classifications by publishing their opinion in the journal Frontiers in Surgery.
EndoGram, which was created in 1995, serves to define the metrics, a sort of ID card of disease. During the first diagnostic laparoscopy, the surgeon takes samples from peritoneal fluid and lesions to identify specific markers of heterogeneity. In order to assure the aggressiveness and progressiveness of the endometriosis for every individual, cell proliferation test, phenotype analyzing using immunochemistry, histological glass slide picture should be performed before deciding the therapeutic program.
This approach will serve to decide the risk of recurrence and the follow-up regiments of the patients; will let to determine the best hormonal therapy depending on the hormone receptor analysis; will allow searching for the best strategy to cure the infertility of the patient, as long as a biological profile for each patient and a true mapping of her disease could be created and a personalized IVF program will be applied.
For an individual mapping, the markers of interest should be those related to angiogenesis, to find the degree of neovascularization and invasion; those related to inflammation as they are important to assess the inflammatory environment, markers of natural killer cells and macrophages to learn about cellular and humoral immunity characteristics. Furthermore, the stem cell markers and the markers concerning proliferation and invasiveness should be delineated.
Certainly, pain and infertility are the major concerns of clinicians for patients with endometriosis. However, before starting to treat the patients, the clinician needs to understand the nature of lesions along with the staging of the disease. Once we have the lesion profile in our hands, we can plan appropriate therapy and avoid excessive use of hormones. Furthermore, this approach may help to assess the risk of malignancy as well.
Research Source: https://www.ncbi.nlm.nih.gov/pubmed/31231658
AFS classification ASRM classification FOATI classification phenotype genotype breast cancer peritoneal fluid hormonal receptors growth factor EndoGram test oncogenic factor endometriosis.

